Why is research on cervical barriers important?
- The HIV pandemic disproportionately affects women and girls. Globally, over half of all people living with HIV are women. Approximately 20.1 million women and girls around the world live with HIV. Young women and adolescent girls between the ages of 10 and 24 years are two times more likely to be infected than boys and young men of the same age. Women and adolescent girls account for one in every five new HIV infections in sub-Saharan Africa. In Russia and Asia, women make up an increasing share of new HIV infections. In the United States, women comprise approximately 19% of new HIV infections.
- Women are biologically more vulnerable to infection and its consequences.
- Gender inequities prevent many women from being able to protect themselves from infection. Violence, coercion, and economic dependency render millions of women unable to negotiate condom use or to leave partners who put them at risk.
Overview
The renewed interest in cervical barrier methods resulted in part from evidence about the role that the cervix may play in HIV/STI transmission. To date, external/male and internal/female condoms are the only barrier methods proven to reduce the risk of HIV/STI infection through sex; however, negotiating condom use remains difficult for people, and scientists are researching potential alternatives to increase prevention options, particularly for receptive sexual partners, and women and girls.
This section presents the relevant information on cervical barriers as potential HIV/STI prevention methods, detailing the biological vulnerability of the cervix and providing information on evidence and research and references on this topic.
Biological Vulnerability of the Cervix
The cervix is the lower opening of the uterus and the gateway to the uterus and the rest of the upper genital tract. It is compromised of three main areas: the endocervix, the transformation zone, and the ectocervix. The vagina and ectocervix, or outer edge of the cervix, are lined with approximately 30 layers of tough squamous cells. In contrast, the endocervix, or the area inside and around the opening to the uterus, is covered with one layer of delicate, columnar epithelial cells. The transformation zone is the area between the ectocervix and endocervix where columnar epithelial cells are replaced by squamous epithelial cells, thus enlarging the ectocervix. This transformation happens rapidly during puberty.
The columnar epithelial cells of the endocervix appear to be particularly vulnerable to sexually transmitted infections (STIs); chlamydial and gonococcal infections are most commonly seen in the cells of the endocervix. The transformation zone is the region most vulnerable to dysplasia (precancerous changes), and research seems to indicate that receptors for HIV are concentrated there as well. In fact, researchers believe the cervix may be the primary site of HIV infection in women.
At the Diaphragm Renaissance meeting in September 2002, virologist Jay Levy and immunologists Dr. Deborah Anderson and Dr. Charles Wira reported on knowledge of the pathways of HIV infection in women. Their research findings implicated the uterus, and thus the cervix, as sites that are particularly vulnerable to HIV infection, largely because many of the receptors known to facilitate HIV transmission (including CCR5 and CXCR4) are concentrated on the cervix. Drs. Anderson and Wira also showed a number of receptor sites in the upper genital tract (uterine endometrium, fallopian tubes, and ovaries), and covering the cervix could also protect these vulnerable areas.
Since HIV can infect people who have had hysterectomies, the cervix cannot be the only site of infection in women. Drs. Anderson and Wira showed that there are HIV receptors in the vagina, and much evidence shows that STIs may cause symptoms (such as sores or lesions) that compromise the vaginal walls and make these areas more vulnerable to HIV infection. Clearly, covering the cervix would likely only provide partial protection from HIV and other STIs.
Evidence and Research
Currently, internal/male and internal/female condoms are the only proven barrier methods to reduce the risk of STI/HIV infection. People who are sexually active and at risk should use a condom every time they have sex in order to prevent HIV/STI transmission.
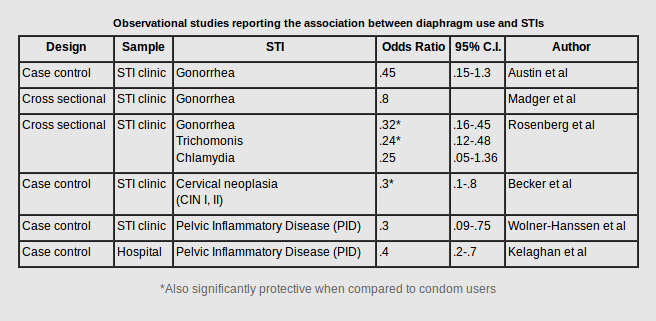
However, negotiating condom use remains difficult for many people, especially women and girls. Therefore, there are a number of studies looking at viable alternatives to provide more receptive partner-controlled STI/HIV options. There were several early observational studies (case-control or cross-sectional designs) that reported that using the diaphragm was associated with a reduced risk of STIs. The table above (adapted from Moench, Chipato, and Padian, 2001) summarizes those results.
The MIRA trial investigated whether the diaphragm would reduce male-to-female STI/HIV transmission. Results did not support the addition of the diaphragm to current HIV prevention strategies. Click here for more information on the MIRA trial.
Additional research on internal/female condoms and cervical barriers is underway and catalogued in our research listings.
Research
Austin H, Louv WC, Alexander WJ: A case-control study of spermicides and gonorrhea. JAMA 1984, 251:2822-4.
Becker TM, Wheeler CM, McGough NS, Stidley CA, Parmenter CA, Dorin MH, Jordan SW: Contraceptive and reproductive risks for cervical dysplasia in southwestern Hispanic and non-Hispanic white women. Int J Epidemiol 1994, 23:913-22.
Cantero-Pérez, J., Grau-Expósito, J., Serra-Peinado, C. et al. Resident memory T cells are a cellular reservoir for HIV in the cervical mucosa. Nat Commun 10, 4739 (2019).
Centers for Disease Control. HIV Surveillance Report, Diagnoses of HIV infection in the United States and dependent areas, 2018. Vol. 30; 2019.
Kelaghan J, Rubin GL, Ory HW, Layde PM: Barrier-method contraceptives and pelvic inflammatory disease. JAMA 1982, 248:184-187.
Magder LS, Harrison HR, Ehret JM, Anderson TS, Judson FN: Factors related to genital chlamydia trachomatis and its diagnosis by culture in a sexually transmitted disease clinic. Am J Epidemiol 1988, 128:298-308.
Moench T, Chipato T, Padian N. Preventing disease by protecting the cervix: the unexplored promise of internal vaginal barrier devices. AIDS 2001;15:1595-1602.
Joint United Nations Programme on HIV/AIDS (UNAIDS). When women lead change happens: Women advancing the end of AIDS. 2017.
Joint United Nations Programme on HIV/AIDS (UNAIDS). Women and HIV: A spotlight on adolescent girls and young women. UNAIDS. 2019.
Padian NS, van der Straten A, Ramjee G, Chipato T, de Bruyn G, Blanchard K, et al. Diaphragm and lubricant gel for prevention of HIV acquisition in southern African women: a randomised controlled trial. The Lancet 2007, 370(9583):251-61.
Rosenberg MJ, Davidson AJ, Chen JH, Judson FN, Douglas JM: Barrier contraceptives and sexually transmitted diseases in women: a comparison of female-dependent methods and condoms. Am J Public Health 1992, 82:669-74.
Wolner-Hanssen P, Eschenbach DA, Paavonen J, et al: Decreased risk of symptomatic chlamydial pelvic inflammatory disease associated with oral contraceptive use. JAMA 1990, 263:54-59.